Grub Soup: It's a can of worms
Guernsey McPearson
Subgroup Analysis: I wasted a term. The Reverend Spooner
'Hallo Guernsey, Your physician is looking for you.' This was from our latest recruit to statistics, Yuri Markov.
He is a pretty serious chain smoker and in consequence exhibits some very ergodic behaviour as he is always on the move
from his desk to the forecourt and back. Rumour is that the powers that be are going to institute a hot desk policy at
Pannostrum, in which case Yuri will be graduating from two states to a random walk. You are always passing
him in the corridor and he seems to have got to know everybody in a remarkably short period. 'Regulator causing trouble with subgroups,' he added.
'Well. I've explained the problem of subgroup analysis umpteen times to Harvey,' I said, referring to Harvey Puffer our earnest 'expert' on all matters pulmonary.
'Did not look much like a "Harvey"', replied Yuri, 'High heels, short skirt, nice hair. Blonde,' he added as an afterthought.
'Either genuine woman or excellent imitation,' he explained raising both eyebrows and smiling conspiratorially. 'Ah,' I said. 'That will be Angina Cutter' and I headed back to the office to pick up my laptop on my way to see our newly promoted head of circulatory.
'Now,' I said to Angina, 'what's all this I hear about subgroups?'
'Gosh, Guernsey. That's sweet. I only just mentioned it to Yuri. Yes, we have a
real issue with our latest trial of lowerstatin. The regulator is asking us to show
that it works in various subgroups. The thing is the result is only just
significant over all.'
'Do they have a trouble with the overall result?'
'No. Not really. This is only an extension into another indication. The mechanism is well
established, as you know it's approved in several indications and the safety record is
pretty solid. They told us beforehand that
one trial would do and they did not mention anything about subgroups at the time.
Now they want us to show that the drug was effective in those also being treated for
hypertension and those who were not. I will admit that we did choose a trial that was a
bit on the small side and the P-value of 0.01 was not that impressive.'
'This girl is a lot brighter than Harvey,' I was thinking, 'give him a P-value of 0.01 and he is cock-a-hoop. But as any statistician
knows if you planned a trial to have 80% power for 5% size and the observed effect is equal to the clinically relevant
difference, you have a non-centrality parameter of 2.8 and that gives you a P-value of 0.005, so 0.01 is,
from one point of view, not as impressive as you hoped.'
'Yes,' I said, 'not terribly impressive but not really inconsistent with what
might be expected from a drug that worked. Of course, I added, if the regulator
requires you to prove significance in each subgroup then the situation is hopeless. It is not even worth looking.'
'Gosh,' said Angina, 'I did not know it was quite so desperate. You mean that there is really no chance.'
'Not really. Have a look at this graph,' I said, showing her my laptop.
'I have this problem programmed up already because the issue arises very often.' I added.
'All I need to do is make the observed P-value 0.01.'
 'Assume that we have the most regular case and that the observed effect is the same in both groups and that the variability
is also the same and that the patients are more or less balanced between the treatment groups within strata.
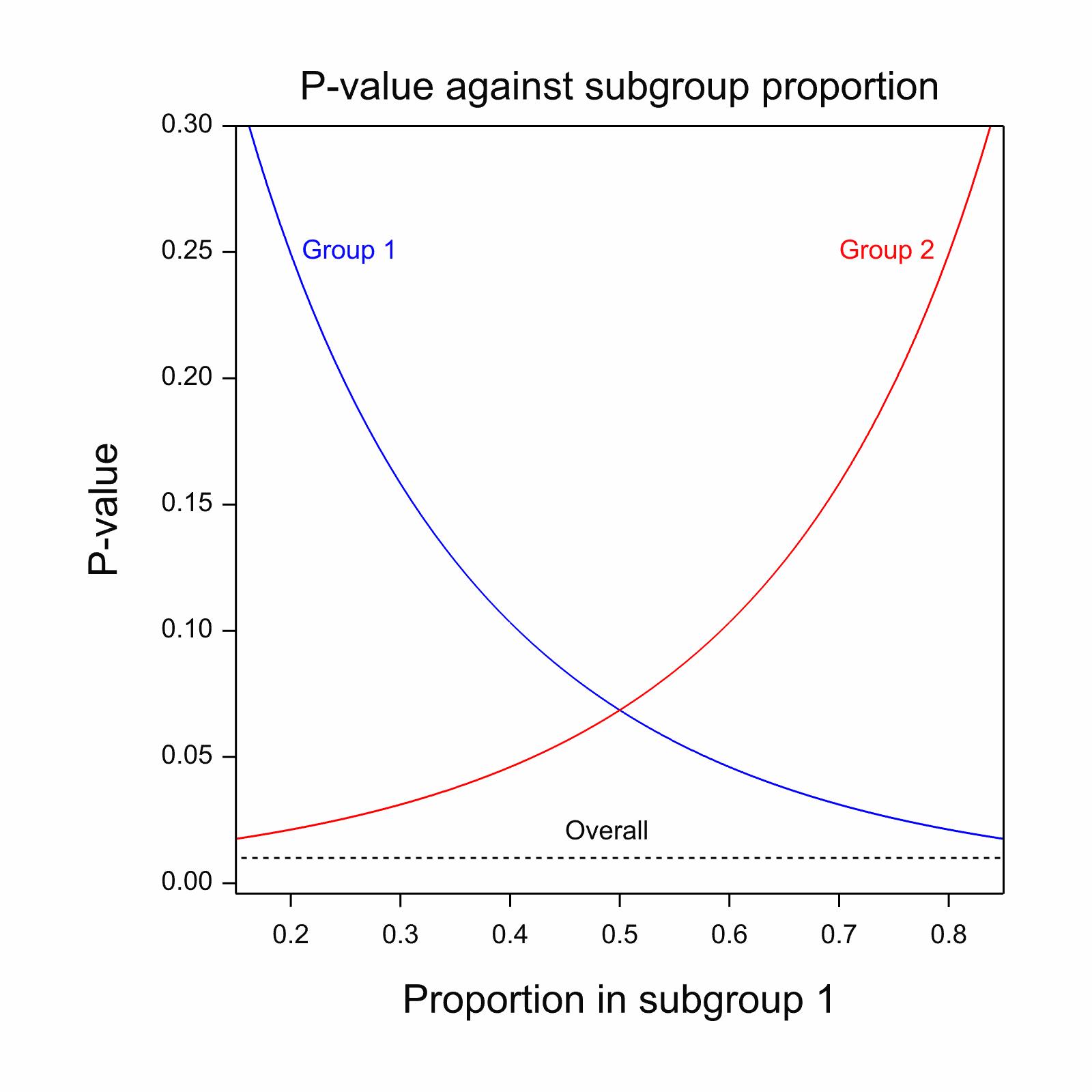
In that case the observed significance in each sub-group will only depend on the sample size. The X-axis shows the
proportion in group 1 and you can plot the two P-values you would see against this.'
'Assume that we have the most regular case and that the observed effect is the same in both groups and that the variability
is also the same and that the patients are more or less balanced between the treatment groups within strata.
In that case the observed significance in each sub-group will only depend on the sample size. The X-axis shows the
proportion in group 1 and you can plot the two P-values you would see against this.'
Angina frowned in concentration 'Oh. I see,' she said, 'the solid blue line shows the P-value in group 1 and I
presume that reaches 0.01 for the case when all the patients are in group 1.'
'Exactly'
'And the solid red line is group 2 and that reaches 0.01 when none of the patients are in group 1 because they are then all in group 2,' she added triumphantly.
'Exactly. And so if you require both subgroups to be significant the best position to be in is to have half
the patients in each sub group and unfortunately that gives you a P-value of about 0.07.'
'So what chance do we have?'
'Only the usual snowball in hell chance,' I added.
'What's that?'
'That the regulators will come to their senses.'
Later I was expounding on the problem to Mrs McP. 'You see,' I said, 'these regulators are obsessed with individual response.
However, often there really is no point in trying to personalise the treatment.'
'Yes, dear' she replied. 'Does that also apply to statisticians dealing with medical advisors?'
Back to GMcP Prose